Skip to content
Skip to content How to Write SOAP Notes? A Guide

You’ve just wrapped up your third counseling session of the day. Your mind is juggling multiple patient stories, treatment plans, and follow-ups. You go back to your notes to plan further for your patients, but they look like puzzle pieces. Now, you’ll have to sit and make sense of all the notes you wrote just because you didn’t follow a specific structure.
Effective documentation is a must for healthcare professionals to keep the records of their patients intact and ensure that they receive better care and collaboration.
Enter SOAP notes. These notes are a structured, time-tested method for clearly, concisely, and actionably capturing client information. The chief complaint is a crucial part of the subjective section of SOAP notes, as it identifies and prioritizes the primary issue or symptom presented by the patient.
Whether you’re a seasoned counselor or just starting, mastering how to write SOAP notes is a skill that can transform your practice. In this guide, we’ll break down the essentials, simplify the process, and help you turn note-taking into a strength, not a struggle.
What Are SOAP Notes?
SOAP notes are a widely recognized and standardized way of documenting client interactions in healthcare, counseling, and other professional settings.
Their structured format ensures that essential information about a client’s condition, progress, and treatment is organized and recorded systematically. This approach promotes consistency and accuracy, making it easier for practitioners to track client care over time and share information with other professionals.
The Four Components of SOAP Notes
SOAP notes are a systematic method for organizing client information. Each component plays a distinct role in providing a complete picture of the client’s condition and progress. Here’s a detailed breakdown of each section, along with practical examples.
1. Subjective (S)
This section captures the client’s perspective, including their feelings, experiences, and statements. It’s often based on what the client directly shares with you.
What to include:
- The client’s self-reported symptoms or concerns, including the client’s chief complaint.
- Specific quotes or paraphrased statements from the client.
- Relevant personal or family history was shared during the session.
- Example:“I’ve been feeling more anxious than usual over the past week. I can’t focus at work, and I’m waking up multiple times during the night,” the client reported.
2. Objective (O)
This section focuses on observable, measurable data that you collect during the session. This might include physical observations, clinical tests, or documented behaviors. Patient notes are crucial for tracking this objective data, ensuring that healthcare providers can make informed treatment decisions by recording observable data and assessments effectively.
What to include:
- Observations of body language or mood.
- Quantifiable data like vital signs or test results.
- Any notable behaviors or changes.
- Example:The client appeared restless, frequently tapping their foot and avoiding eye contact. During the discussion, they rated their anxiety as 8 out of 10.
3. Assessment (A)
In this section, you analyze the subjective and objective information to form a professional interpretation. This may include progress evaluations, diagnostic impressions, or changes in the client’s condition. It is also crucial to document the present illness, detailing how the patient’s situation has developed, including their symptoms, medical history, and relevant treatments.
What to include:
- Your interpretation of the client’s reported symptoms and observed data.
- A summary of progress or setbacks.
- Any working diagnoses or hypotheses.
- Example:The client is exhibiting signs consistent with generalized anxiety disorder (GAD), including restlessness, difficulty concentrating, and sleep disturbances. Symptoms appear to have worsened since the previous session.
4. Plan (P)
The plan outlines the next steps in treatment, including goals, interventions, and follow-up actions. It provides a clear roadmap for addressing the client’s concerns.
What to include:
- Specific treatment goals.
- Interventions or techniques to be applied.
- Any referrals, medications, or follow-up appointments.
- Relevant client behavior, including personal insights and goals related to their health and rehabilitation.
- Example:
- Introduce deep breathing exercises to manage anxiety.
- Schedule a follow-up session in one week to monitor progress.
- Encourage the client to maintain a daily journal to track sleep patterns and triggers.
- Refer to a travel occupational therapist who can visit them at home and teach them coping mechanisms to deal with anxiety.
Here’s how a complete SOAP note might look:
| Subjective: The client stated, “I feel overwhelmed at work and can’t seem to keep up. My chest feels tight when I think about my deadlines.” Objective: The client presented with a tense posture and frequent sighing and reported a headache rated 6/10 in severity. Assessment: Symptoms suggest increased stress levels contributing to physical tension and difficulty concentrating. Plan: – Teach relaxation techniques during the next session. – Recommend reducing caffeine intake and incorporating short breaks during work. – Follow up in two weeks to assess stress levels and headache frequency. |
|---|
How to Write Effective SOAP Notes
Writing SOAP notes doesn’t have to feel like a chore. With the right strategies, you can make the process efficient and ensure your notes are clear, professional, and actionable.
Let’s break down how to write soap notes for counseling step by step:
1. Start Immediately After the Session
The best time to write SOAP notes is immediately after your session. Waiting too long can result in forgotten details or less accurate recollections.
Details are freshest right after a session. Writing your notes promptly helps you capture subtle nuances, client statements, and observations that might fade with time. Block out a few extra minutes at the end of each session specifically for note-taking. Including the patient’s medical history in your notes is crucial for informed clinical reasoning and thorough patient evaluations. Think of it as a key part of your workflow, not an afterthought.
2. Keep It Clear, Keep It Concise
SOAP notes aren’t meant to be essays. They should convey the necessary information without unnecessary elaboration.
Ambiguity or overexplaining can lead to confusion or misinterpretation. Clarity ensures that other professionals reviewing the notes can quickly grasp the situation. For each section, use bullet points or short, structured sentences. Avoid jargon or overly technical language unless it’s essential. Include pertinent family history without unnecessary details to ensure relevance to the patient’s diagnosis and treatment.
3. Leverage Note Taking Apps
Using digital note-taking tools can make SOAP notes easier to organize, edit, and share across teams. Digital platforms designed for documentation and collaboration offer the structure and efficiency needed to keep notes consistent and accessible.
Nifty, for instance, provides pre-designed templates specifically tailored to organize information in a structured format. These templates make it simple to maintain accuracy while saving time. Using a standardized SOAP note template enhances healthcare service quality by ensuring efficient documentation, organization, and compliance.
These tools don’t just improve note-taking; they transform how you manage client information. With Nifty, you can populate the Subjective, Objective, Assessment, and Plan sections effortlessly, ensuring every critical detail is documented without unnecessary stress. The collaborative features enable seamless communication, allowing team members to access and update notes in real time while maintaining a secure environment.
Storing notes within a centralized digital platform also safeguards client confidentiality. Nifty organizes all documentation in one place, ensuring compliance with privacy standards while allowing you to retrieve and review information instantly.
4. Refine, Review, Repeat
Writing SOAP notes isn’t a one-and-done process. Regular review ensures accuracy and allows for adjustments based on the client’s progress. Progress often unfolds over time. Reviewing notes can help you track patterns, refine your assessments, and adjust plans more effectively.
Set aside time each week to review past notes. This habit improves note quality and helps you prepare for upcoming sessions. Progress notes play a crucial role in tracking client progress and refining treatment plans, ensuring that any necessary adjustments are made in a timely manner.
5. Stay Objective and Avoid Assumptions
SOAP notes should be factual and free from assumptions or emotional bias. Notes are part of a client’s medical record and may be reviewed by other professionals or even in legal settings. Staying objective ensures professionalism and credibility.
Avoid statements like “The client is lazy” or “They seem uninterested.” Instead, describe observable behaviors: “The client did not complete the assigned tasks and stated they lacked motivation.”
6. Ensure Confidentiality and Security
Confidentiality is non-negotiable when it comes to SOAP notes. Ensure that your records are secure and comply with legal and ethical standards. Protecting client information is not only ethical but also often required by law, such as HIPAA regulations in the U.S.
Use password-protected devices and encrypted apps for digital notes. If you’re using paper, store them in a locked, secure location. Avoid discussing details in non-secure environments.
Streamline your SOAP note process with Nifty
Get Started
Benefits of Using SOAP Notes
SOAP notes are an essential tool for maintaining high standards of care and ensuring consistency in documentation. Here’s a closer look at how they can transform your practice:
1. Clarity and Organization
SOAP notes provide a structured format that organizes information into clear categories: Subjective, Objective, Assessment, and Plan.
This ensures that all critical details, from client-reported issues to actionable next steps, are documented systematically. By breaking down information into these sections, SOAP notes reduce confusion and help you focus on the most relevant details.
2. Improved Communication
Whether you’re collaborating with colleagues, referring a client to another professional, or preparing for a team discussion, SOAP notes offer a universal format that is easy to understand.
Their concise yet detailed structure ensures that everyone involved in a client’s care can quickly grasp the situation. This includes other healthcare professionals, who benefit from enhanced visualization of patient notes and treatment plans, supporting collaborative patient care.
3. Progress Tracking
SOAP notes create a chronological record of a client’s journey over time. By comparing notes from different sessions, you can identify patterns, measure progress, and assess the effectiveness of interventions. This is especially useful when adjusting treatment plans, such as when prescribing Zepbound for weight loss, so as to monitor and adjust the treatment based on the client’s progress.
4. Legal Protection
Accurate documentation isn’t just helpful—it’s often a legal requirement. SOAP notes provide detailed, objective records that can serve as evidence in case of legal disputes, audits, or insurance claims.
The structured format ensures that your notes meet professional and legal standards, protecting both you and your clients.
5. Enhanced Decision-Making
SOAP notes give a comprehensive view of the client’s situation by separating subjective client input from measurable objective data and pairing it with your professional assessment.
This layered approach allows you to make more informed decisions about treatment plans and next steps, improving the quality of care you deliver.
6. Time Efficiency
Writing notes can often feel time-consuming, but the standardized SOAP format streamlines the process.
You know exactly what to include in each section, eliminating guesswork and reducing the time spent on documentation. Over time, this efficiency frees up more time for client interactions and other important tasks.
Common Mistakes to Avoid While Writing SOAP Notes
Even with the best intentions, errors in SOAP notes can undermine their effectiveness. Recognizing and addressing these common mistakes is crucial for creating precise, actionable records. Here’s what to watch out for:
Mistake 1: Overloading Notes with Unnecessary Details
Providing excessive or irrelevant details can make your notes cluttered and difficult to follow. For instance, writing a paragraph about the client’s unrelated hobbies instead of focusing on their presenting concerns dilutes the value of your documentation. Stick to the SOAP framework and focus on information directly related to the client’s condition or treatment. Adhering to the soap note format ensures clarity and thorough documentation, which is crucial for guiding patient management and facilitating effective treatment strategies within the healthcare setting.
How to avoid it
- Stick to the SOAP framework and focus on information directly related to the client’s condition or treatment.
- Use concise, targeted language, avoiding over-explanations or irrelevant anecdotes.
- Regularly review notes to ensure they remain clear and to the point.
Mistake 2: Missing Critical Information Due to Rushed Documentation
In a hurry, it’s easy to leave out important details like specific symptoms or observations. For example, failing to document a client’s reported sleep disturbances can hinder accurate assessment and planning.
How to avoid it
- Allocate time after each session specifically for note-taking.
- Use templates to ensure all critical sections are addressed.
- Practice active listening during sessions to capture key details effectively.
Mistake 3: Using Vague Terms or Unverified Data
Phrases like “the client seems upset” or “likely improving” lack clarity and precision, making the notes less reliable for decision-making.
How to avoid it
- Describe observable behaviors or measurable outcomes instead of subjective impressions. For example, write “The client appeared tearful and reported feeling sad daily for the past week” instead of “The client seems upset.”
- Verify details with the client before documenting.
Mistake 4: Skipping the Review Process for Accuracy and Clarity
Failing to review notes can result in errors, omissions, or inconsistent language, which can confuse other professionals or lead to legal issues.
How to avoid it
- Set aside time after writing to review and refine your notes.
- Check for grammar, spelling, and accuracy in details.
- Ensure the notes align with professional and legal standards.
Best Tools for Writing SOAP Notes
Using the right tools can significantly improve the efficiency and quality of your SOAP notes. These tools offer templates, collaborative features, and secure storage to simplify your documentation process. Here are three excellent options to consider:
1. Nifty
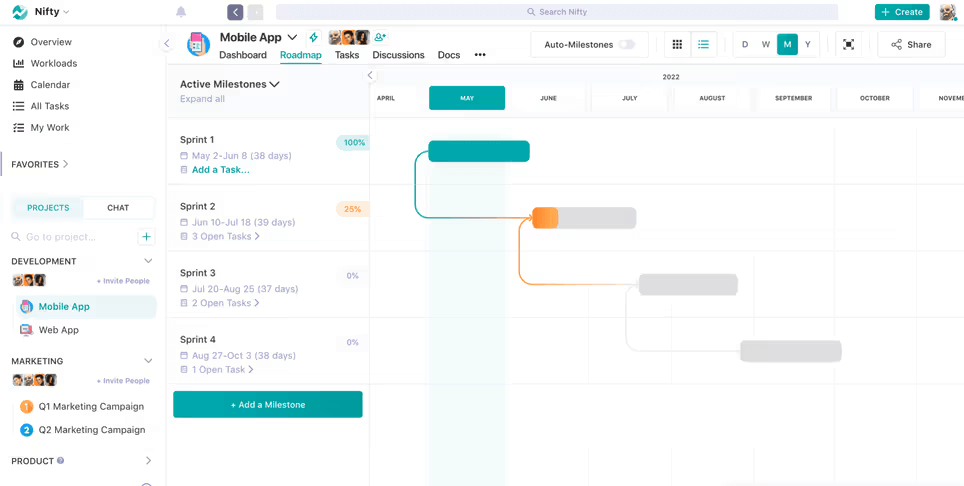
Nifty is a powerful project management tool that streamlines the process of writing SOAP notes. Its customizable templates and collaborative features allow professionals to maintain organized, accurate, and accessible documentation. These features enable healthcare providers to align on treatment plans, document clinical reasoning, and ensure coordinated care.
The centralized workspace securely stores all notes, action items, and client data in one place. Its real-time collaboration tools also make it easy for teams to collaborate on client care plans.
Key Features
- Pre-designed templates for structured documentation.
- Real-time collaboration and sharing.
- HIPAA-compliant secure storage with encryption for client confidentiality.
Simplify SOAP notes with Nifty!
Get Started
2. SimplePractice
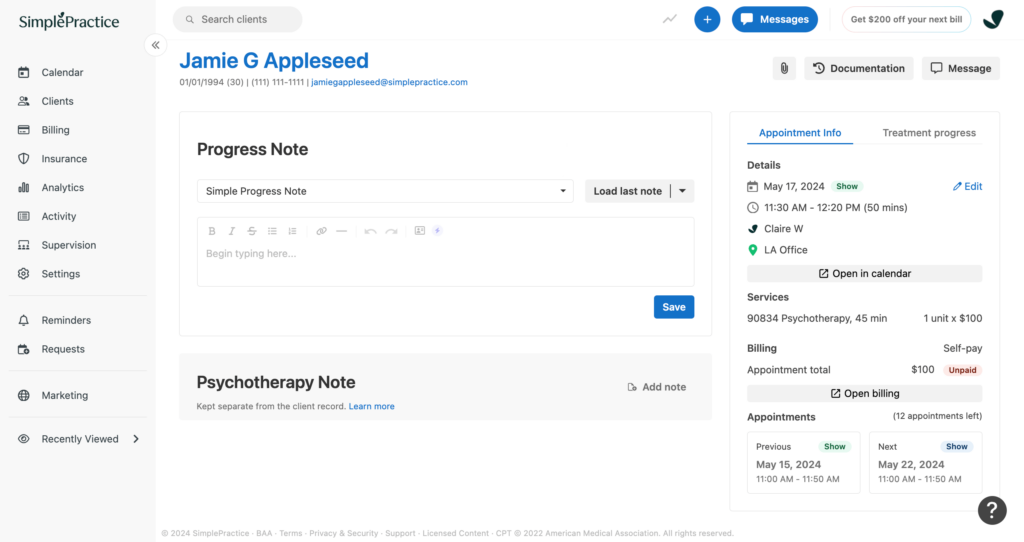
SimplePractice is a comprehensive practice management tool designed specifically for therapists and counselors. It includes built-in SOAP note templates that are easy to customize and integrate seamlessly with client profiles. The platform also offers scheduling, billing, and telehealth features, making it a one-stop solution for private practices.
Key Features
- Ready-to-use SOAP note templates tailored for mental health professionals.
- Integration with client records and appointment schedules.
- HIPAA-compliant storage and security.
3. TherapyNotes
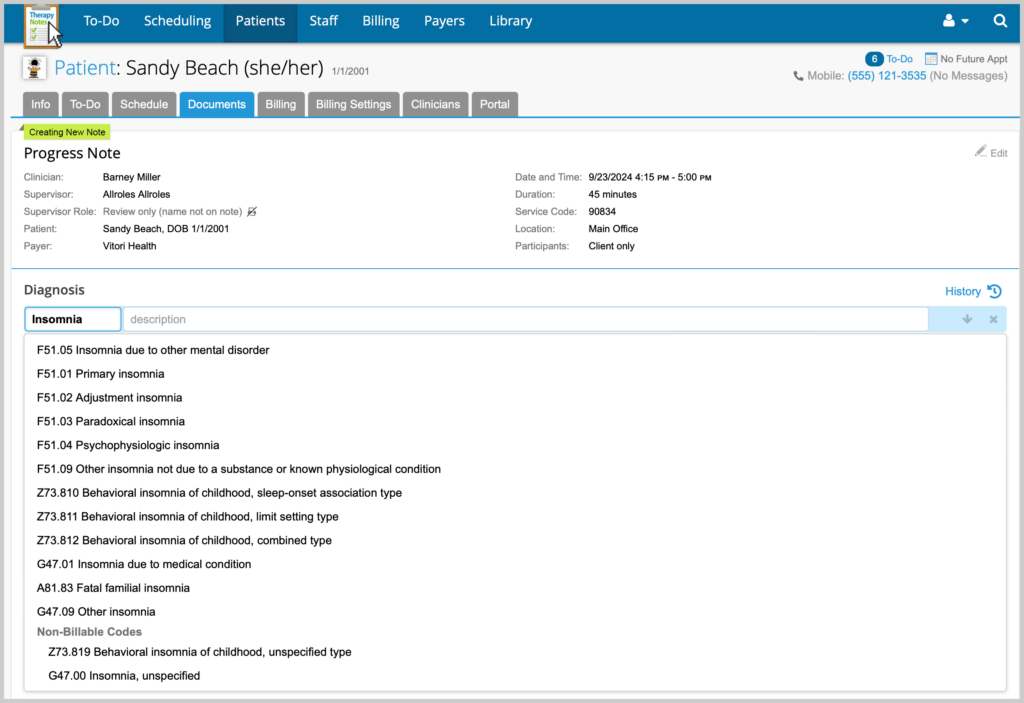
TherapyNotes is another excellent platform for mental health professionals. It provides a user-friendly interface for writing and organizing SOAP notes, along with features for scheduling, billing, and managing client records. Its secure cloud-based storage ensures that notes are accessible from anywhere while maintaining privacy standards.
Key Features
- Structured SOAP note templates with customizable options.
- Comprehensive client management system.
- Cloud-based, HIPAA-compliant storage for accessibility and security.
Turn SOAP Notes into Your Secret Superpower With Nifty
Writing SOAP notes isn’t just a routine—it’s a skill that can redefine how you approach client care. Beyond documentation, these notes bridge understanding your client’s needs and delivering meaningful outcomes. Mastering this method equips you with a powerful tool to make informed decisions, track progress, and collaborate effectively.
The right tools, however, make all the difference. Nifty steps in as more than just a note-taking app—it’s a transformative platform that brings clarity, consistency, and ease to your workflow. With templates, secure storage, and collaboration features, Nifty takes the guesswork out of documentation, leaving you free to focus on your clients.
Ready to elevate your practice? Start simplifying your SOAP note process with Nifty today and discover how organized documentation can unlock your full potential. Try Nifty for free and see the difference!